

From late April to early May 2026, we visited medical facilities in three Bangladeshi cities (Dhaka, Narail, and Cox’s Bazar) and a Rohingya refugee camp.
The objectives of this visit were as follows:
- To observe the health problems faced by people, especially pregnant women and children, living in the Rohingya refugee camp, one of the world’s largest refugee camps housing over one million refugees, and to identify matters where health support is lacking.
- To examine the medical situation and challenges within Bangladesh, particularly in Cox’s Bazar, which has accepted such a massive number of refugees.
- To examine the health problems faced by people in Bangladesh in cities other than Cox’s Bazar.
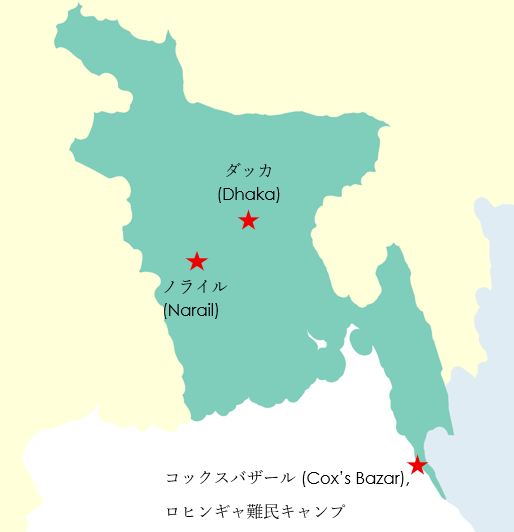
As shown in the map below, we visited three Bangladeshi cities: Dhaka, Cox’s Bazar, and Narail.
We also visited the Rohingya refugee camp in Cox’s Bazar.
We visited a private children’s hospital and a university hospital in Dhaka, as well as district and public hospitals in Cox’s Bazar and Narail, with a primary focus on neonatal and pediatric wards and delivery rooms. In some hospitals, we were also allowed to observe adult wards.
Here are three main problems we observed:
Insufficient Hospital Beds
Every hospital was overflowing with patients, especially in rural areas where there were 10 times more inpatients than available beds. Due to the overwhelming shortage of beds, many patients were receiving IV drips on mats laid out in the corridors.
In rural areas, even in the largest hospitals, such as district hospitals, 3 or 4 newborns and pediatric patients shared a single bed, with their accompanying mothers and other family members sitting nearby on the same bed.
Shortage of Medical Staff
Doctors often make rounds on the wards in the morning and head to their clinics in the afternoon. This leaves the remaining nurses struggling to provide patient care when they have difficult cases.
This is due to low hospital salaries, which lead doctors to prioritise higher-paying clinics, in addition to a shortage of doctors.
This is a common sight not only in Bangladesh but also in other Asian and African countries where there is a shortage of doctors.
The Burden of Medical Costs
National and public hospitals are always overcrowded, as described above. Therefore, those who cannot be hospitalised or receive treatment, and who can somehow afford it, go to private hospitals or clinics.
The private children’s hospital we visited was far more stable in terms of medical equipment and staff numbers, compared to the national hospital. However, for example, the cost of hospitalisation for a newborn is at least 9,000 yen per day, and in Bangladesh, where the average monthly salary is 20,000 yen, very few patient families can afford this medical expense.
Furthermore, one characteristic of healthcare in Bangladesh is the high prevalence of cesarean sections; some facilities report that 70% of the total deliveries are performed via cesarean section. The reasons are varied, including hospital profitability, the convenience of being able to plan cesarean sections, and the fact that many patients prefer cesarean sections.


The Rohingya refugee camp is currently the world’s largest refugee camp, with approximately 1.2 million refugees living there. The population density is extremely high (more than six times the density of Tokyo).
About 50% of the total population are children, and including women brings the figure to about 80%, meaning that the vast majority of the camp’s inhabitants are women and children.
The houses are simple structures made of wood and plastic sheeting.
There is no electricity, and although we frequently saw solar panels placed on the roads, the amount of power they can provide is negligible.

There are no “schools” within the camps; instead, each camp has learning centers built by NGOs and other organisations.
These centers offer classes in several subjects like mathematics and English, but due to financial difficulties and other factors, the education provided to children looks inadequate.

The type of medical facilities within the refugee camps is mainly divided into three categories.
Of these, the following two facilities are the most accessible to the people.
| Health Post | Primary Health Center | |
| Total number of facilities in the entire camps | 46 | 46 |
| Staff | Medical assistants, nurses, midwives, etc | Doctors, nurses, etc. |
| Service | common cold treatment, vaccinations, antenatal checkups, etc | Delivery, trauma care, and mental health, etc |
Those who cannot be treated here are taken to larger hospitals run by the UN and NGOs. These hospitals are located within the camp or at the border with the host community, so that people from host communities can also be treated.
Currently, there are approximately five hospitals capable of providing delivery service and neonatal care, including those run by MSF and IOM.
Among the many challenges here, let’s highlight three issues related to the medical care of pregnant refugees and children.
Risk of home delivery
Traditionally, Rohingya refugees tend to prefer home delivery and often do not come to hospitals for antenatal checkups. Therefore, the overall picture, such as the total number of pregnant women in the refugee camps, is often unclear.
However, some estimates suggest that about half of the pregnant women in the camps choose home delivery and prefer traditional midwives (TBAs).
Furthermore, data show that the majority of maternal deaths in the camps occurred during home delivery assisted by TBAs, highlighting the need to improve the knowledge and skills of TBAs.
Currently, IOM and UNFPA are focusing on encouraging antenatal checkups, while also providing training for TBAs and collaborating with them.
Lack of newborn and infant Health Checkups
Health checkups for newborns and infants, which are commonplace in Japan, do not exist here. Therefore, the development of children, including physical development and the development of motor skills, language, social skills, and cognitive functions, is unknown.
Parents only bring their children to health facilities if they suspect illness. It means that a child’s health depends heavily on the parents’ awareness.
Adolescent Depression
While mental health issues such as anxiety and depression are said to be a major problem in the Rohingya refugee camps across all ages, the doctor I spoke with expressed great concern about adolescent depression and anxiety.
Causes cited include domestic violence, anxiety about an uncertain future, and so on.
They sometimes have access to the internet and see the lives of other children of their age in the world online. Comparing their own lives to others might cause their anxiety.
These are medical and health issues for refugees living in refugee camps, but the medical situation for people in the nearby host communities is not significantly different.
Because there were originally no facilities for pregnant women in the host communities to be hospitalised, they now receive treatment at hospitals built for refugees by international organisations.
We had a chance to visit the work site of Artolution (https://www.artolution.org/), an American NGO. who have been working in the Rohingya refugee camps since 2017, when a large number of Rohingya refugees entered Bangladesh.
In addition to providing psychological support to children through craft activities at a learning center within the camp, they are also carrying out wall art projects in the host communities as well as within the camp.


